Welcome to WordPress! This is your first post. Edit or delete it to take the first step in your blogging journey.
📄 CASE STUDY: FALLING THROUGH THE CRACKS IN WALES
One Year On – A System That Is Failing
Background
This case concerns a 50 odd -year-old woman with a diagnosis of Autism and history of clear Mild Learning Disability. She has an IQ of 72, placing her in the critical “in-between” category. She has complex physical health needs, including suspected Ehlers-Danlos Syndrome (EDS) / Hypermobility, chronic pain, spinal issues, and digestive problems. (Asked for investigations failed now aware fits criteria)
She moved to Wales from England one year ago expecting continuity of care. Instead, she has experienced a complete breakdown of support, misdiagnosis, and a system that relies on outdated practices. The study includes links and resources to support the case study.
1. AGING AND LIFE EXPECTANCY – A MATTER OF LIFE AND DEATH
At 50 odd years old, this individual has already done well to reach this age. With the right support in England recognised.
– Family History: Many members of her family died between the ages of 40 and 62.
– Autism Statistics: Research confirms that autistic people have a significantly reduced life expectancy. For autistic women with a learning disability, the average life expectancy is just 69.6 years – meaning she may have very limited time left.
– The Risk: When needs are not met, life expectancy drops further. Just like someone diagnosed with cancer who chooses treatment to prolong life, this individual wants to live her life to the full – but she cannot do this alone. Without the right support, years are being taken off her life.
Source: https://pmc.ncbi.nlm.nih.gov/articles/PMC10769892/
2. THE IQ LABEL – A NUMBER THAT IGNORES REALITY
In England, an IQ between 70-75 is widely recognised as indicating a mild learning disability, triggering support and health checks. Social Services are set up to understand this type of learning disability with their autism too, plus trained and influence by the Oliver’s campaign.
In Wales, the cut-off is strictly 70.
Because this individual scores 72, they are deemed “not eligible” despite clear evidence of:
– Severe dyslexia
– Well below average ability in all functional areas
– Difficulty with time, numbers, reading, and writing
– Executive dysfunction – inability to plan or organise daily life
Proof of Need Throughout Life:
– From the age of 8, she was under the care of Mencap clubs and use in England and campaigning group for Mencap England and attended SEN schools in the 1970s and 80s.
– Even playgroup/pre-school could not cope with her needs, requiring private childcare to prepare her for school.
– She was placed in classes with both severe and mild learning disabilities, where needs were often hard to recognise.
– At high school and college, she was fully segregated from mainstream education in mainstream settings and left without GCSEs – yet today, many people with lower IQs achieve these qualifications. This lady did go back to college to learn a basic English of maths but actually could not learn any more than she could have learned in school, tried very hard on different occasions and got nowhere.
– She successfully drove a car for many years, proving that a label does not define ability – yet old care plans incorrectly stated “people with learning disabilities cannot drive”. Recently online you can see that a down syndrome has passed his test and the first person to pass a test or someone in Ireland, which shows there’s no limits to what people can do with the learning disability even under 70 cut off point! There is one in her madcap campaigns that can drive, and one I won back in England used to drive them Mencap bus to pet people up in the community to attend the clubs.
The Reality:
IQ tests are not perfect. This assessment was done years ago, before an autism diagnosis, and did not take into account anxiety or processing differences. A number cannot measure a whole person. Clearly returning to England and again had substantial support raising her children this is documented in social services assessments in England.
Source: https://www.psychiatry.org/patients-families/intellectual-disability/what-is-intellectual-disability
3. MISDIAGNOSIS AND OUTDATED LABELS
The individual has a history of trauma, including rape at 16, which led to self-harm and admissions to hospital.
– In the 80s, 90s, and 2000s, she was sectioned and diagnosed with “Personality Disorder”.
– She was heavily medicated, which caused long-term gastric damage.
– Today, it is recognised that this was NOT personality disorder – it was undiagnosed Autism. Raising children a social worker clearly stated she was more like an older sister to them, rather than a parent suggesting possibly intellectual disability, with all the right support she was able to raise her children with much support from most services including services in our home.
The Problem in Wales:
Professionals still use terms like “Mental Health” and “Neurodiversity” as a blanket term. They fail to look at Autism specifically.
– They confuse communication differences (talking at length, going off-topic) with “behaviour problems”.
– They suggest speech therapy, yet the individual speaks perfectly clearly – they just need people to guide them back to the topic gently.
– They are using old models of care instead of modern autism understanding.
Source: https://www.nationalelfservice.net/learning-disabilities/autistic-spectrum-disorder/autistic-adults-bpd-misdiagnosis/
4. RAISING A FAMILY – LOVE, SUPPORT AND INHERITED NEEDS
This individual raised 3 children 2 from a marriage that clearly didn’t work out because her husband had autism and severe mental health disabilities it would have been impossible for it to raise children in that environment, she decided to divorce him herself which shows a lot of courage are in children hasn’t seen their father since either. Social workers at the time noted she was “more like an older sister” and needed significant support – yet she was trusted completely and did an amazing job.
– The Inheritance: All her children are on the SEND/Additional Learning Needs register.
– The Spectrum: They are all different. Her daughter works and lives independently, raising her own child with additional needs. Her two sons have similar needs to her own – autism and mild learning disabilities – one needing more support than the other.
– The Lesson: This proves that needs are individual. You cannot put people in boxes. Each person requires their own plan based on their own abilities and challenges.
5. THE TRAGIC LESSON OF OLIVER MCGOWAN – WHY TRAINING MATTERS
Oliver McGowan was a young man with autism and mild learning disabilities. He attended mainstream school, passed his GCSEs, and was ready to live independently with minimal support.
– He had capacity and clearly told staff not to give him certain medications because of side effects.
– His autism was treated as “behaviour”. He was given medication against his wishes and against his parents’ advice.
– He suffered severe brain damage and died as a result.
This could happen to anyone. Mistakes are made because staff do not understand, do not listen, and see autism as a problem to be managed rather than a way of being.
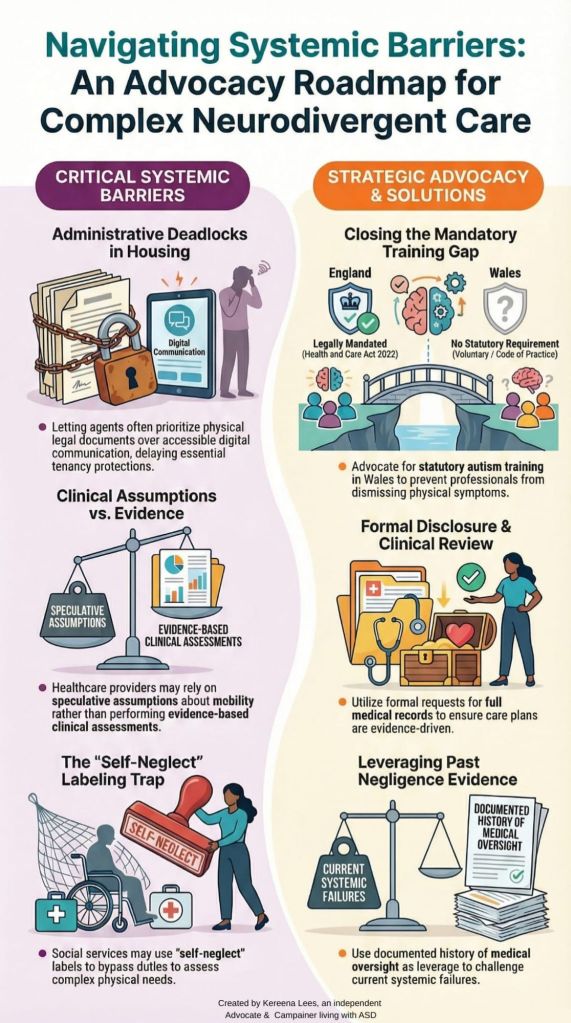
England vs Wales:
– In England: Since 2023, the Oliver McGowan Mandatory Training is compulsory for all health and social care staff. It teaches them to listen, understand communication differences, and make reasonable adjustments.
– In Wales: The system uses different training, often focused only on people with severe learning disabilities.
– In Conwy: The “Healthcare Champions” and liaison nurses are trained – but you often need to have an IQ below 70 to access their support fully. People with IQ 70-75 are left behind, even though they have clear learning disabilities and complex needs.
The Solution:
Wales must adopt the Oliver McGowan training and ensure it covers all levels of learning disability and autism. We must stop separating them and start seeing the whole person. Including the Paul’s foundation in Wales. One includes mild learning disability the other severe learning disability. Link in these together in mandatory training could be very useful across Wales, to prevent unnecessarily more cases of individuals that clearly needs support or on the learning disability register.
Source: https://www.hee.nhs.uk/sites/default/files/FAQs%20for%20The%20Oliver%20McGowan%20Mandatory%20Training%20on%20Learning%20Disability%20and%20Autism%20-%20Feb%202024.pdf
6. PHYSICAL HEALTH – A TICKING TIME BOMB
The individual suffers from:
– Chronic Pain: Reletrans patches (10mg) are now at the maximum dose a GP can prescribe – usually reserved for cancer patients – just to manage daily pain.
– Bone & Joint Issues: Degeneration, swelling in arms/legs, nerve pain, and a history of being a dancer (common in hypermobility).
– Digestive Crisis: Severe constipation, Hiatus Hernia, Reflux, Fatty Liver, and Pancreatic issues.
– Sensory Eating Issues: Has only ever eaten specific foods safely. Without support to cook or shop, diet is poor, leading to vitamin deficiencies and weight loss.
The Failure:
– Scans and ultrasounds miss internal damage. An Endoscopy and Colonoscopy are vital but are being delayed.
– Because of Autism, they require General Anaesthetic or Deep Sedation for procedures – this reasonable adjustment is being ignored.
– Altered Pain Perception: The brain does not signal pain correctly, meaning injuries and illnesses are missed until it is too late. This puts the individual at extreme risk – similar to the cases of Oliver McGowan and Paul Ridd.
Source: https://www.bsms.ac.uk/about/news/2026/new-study-reveals-high-rates-of-likely-undiagnosed-autism-and-adhd-in-people-with-chronic-pain-and-fatigue.aspx
7. SOCIAL SERVICES – BREACHING THE WELL-BEING ACT
Despite the Social Services and Well-being (Wales) Act 2014 stating that needs must be met regardless of label:
– Assessments are taking months/years.
– The assessor has written a care plan/assessment without showing it to the individual first same has last year. (Seen the care plan from last year, was clearly unfounded) A GP in Wales as clearly identified with the expert knowledge, but says your services seems to need more evidence which obviously is taken a very long time with their old system, clearly if any doubt support should be put into place and reasonably made clearly not in this case. Clear things has escalated with a physical health. Along with new conditions with lack of support to even follower diet plan to prevent it getting worse, when the client cannot cook a four meal safely in a kitchen regardless to a physical health needs in fact before she even was a wheelchair user, she needed the support to be able to cook a basic meal at home for her and her children. If this individual could cook alone, she would never have needed the support throughout the years. There’s now assessment this year is clearly based on all needs including a physical needs. But it’s not just about the safety in the kitchen now it’s always been there whether in a wheelchair or not.
– They focus on “teaching independence” despite a lifetime of evidence showing 24/7 support is required. Which can take some time to complete and get to know their client. In recent evidence social services in Wales as clearly taken children from families very quickly, because of the way they were in their system in England that has never been the case, there’s quite a few people within Leicester that raises children independently with substantial support around them just as in this case.
– They downgrade needs, claiming the individual “can do more” while ignoring medical evidence from GPs and specialists. Throughout the years this lady has been through this many times and could have lost their children, the system in England is far different got the lady back on to track, gave her a support back, because clearly, she would not have been able to raise the children without and give them a quality of life to get them to where they are today.
– Telecare / Alarm System: They are being told they must pay, yet this should be free under a care plan if living alone and at risk of falls.
The Result:
– No help with cooking, cleaning, for filling easy read letters or shopping. HOW MUCH MORE.
– Health is deteriorating rapidly. If a care plan was in place after all this time, I need would be changing more especially with the cataracts found. And again for reasonable adjustments to have them fixed for a better quality of life, not under just local anaesthetic as can be risky for the individual and clearly the surgeons trying to do it because of all our sensory issues it would possible and dangerous.
– The individual is in Autistic Burnout – sleeping until 1pm, missing alarms, exhausted by pain and fighting the system. Showing that needs a complex and getting worse because of the big changes in their life from having support to none. Impacting of mental health, I mental health have been clear there won’t help the client pushing them back to social Services each time and assessment has been done over the last year. Clearly that is evidence in itself. No actual mental health that all down to the autism side, mental well-being is more of a priority and supporting all her needs.
Source: https://www.legislation.gov.uk/id/anaw/2014/4/section/19
8. HOSPITAL & A&E EXPERIENCE
The individual is now terrified to go to hospital.
– Overcrowding and long waits cause sensory overload.
– Staff do not understand autism or reasonable adjustments. Letters back from from consultants are evident of this using the term mental health or argumentative behaviours, when she’s clearly trying to express her rights to treatments. That I clearly not going to happen without the right support in place.
– Physical needs are often dismissed, or overshadowed by assumptions about mental health all the blanket system because of the personality disorder she was diagnosed with gets crossed with her autism needs when clearly it should be pushed down into pass records to concentrate on supporting autism needs and physical health. And social inclusion, the client spends more time on our own in a property, accessing things she really wants to do and has gifts in. ( Where are her rights when she says “what’s important to me)”! As it stands this is not being met either.
– They end up discharging themselves just to escape the overwhelming environment. Or over talk being distressed and it’s a coping mechanism. Sadly no one’s actually ear in the individual, they just say mental health issues or attention seeking.
– Outcome: Tests are not done, problems are missed, and the individual is sent home to suffer.
This is dangerous. People are dying waiting for treatment in Wales. With additional needs or not, yet everyone with a learning disability under 60 gets more rights and privileges on the learning disability register. Which can help diagnose any health needs before they arise and get the important treatment that goes along with it so no more mistakes get made in health. Yeah this individual falls between the gaps in Wales.
Source: https://www.walesonline.co.uk/news/health/one-biggest-problems-welsh-nhs-32733471
CONCLUSION – ONE YEAR ON
One year after moving from England, where support was in place and understood:
✅ Liaison Nurses
✅ Digital Flags on records
✅ Annual Health Checks
✅ Home Care Support
In Wales, there is nothing. Even when a GP flags her communication and altered pain perception needs into the equation. Under hospital passport that never gets read very rare by the ambulance service. Just for reasonable adjustments. But no liaison or support to implement them only once! The last time she was ever at A and E. The because she is not under them the hospital’s staff completely ignored even a small amount of support from them. Completely traumatized her. And had to get therapy herself to talk about it. With knowledge of altered pain perception underneath with her autism.
The system is outdated. It hides behind words like “Neurodiversity” and “Mental Health” to avoid doing the actual work. It uses an IQ number to deny rights to people who clearly need help. But actually fall under the category for learning disability.
This individual is deteriorating physically and mentally. They are at high risk of becoming another statistic.
This is not an isolated case. There are many “In-Betweeners” in Wales suffering in silence because they do not know how to fight. So this is written from one of the wore cases the whole of Wales. Weather is very clear need. Moving borders in the UK.
RECOMMENDATIONS & DEMANDS
1. Stop using IQ as a pass/fail test. Assess needs based on what the person can and cannot do, history of support, and daily functioning. Recognise that 70-75 is a valid range for mild learning disability.
2. Adopt the Oliver McGowan Training Nationwide. Ensure all staff in Wales are trained to understand both autism and learning disabilities at all levels, and learn to listen to what people are saying.
3. Retrain Staff. Stop confusing Autism with Mental Health or Behaviour. Understand communication differences.
4. Investigate Physical Health Properly. Arrange the Endoscopy/Colonoscopy with full sedation. Test vitamins and minerals.
5. Implement Support Immediately. Do not wait years for assessments. Put care in place to stop further health decline and improve quality of life.
6. Follow the Law. Comply with the Well-being Act and provide Telecare and home help as required.
This case is evidence that the system in Wales is broken for people who fall in the gaps. Change must happen now before it is too late.
This kind of thing needs to be shared all over wales, especially to social services and the natural health boards. Whether the case or individual is recognised or not from our case study. It was too hard not to put a details into it all, she fully understands this. To bring the case study to life.
My my own case study with support.








Leave a comment